THEY ARE NOT ALONE FOUNDATION
CONTACTS
THEY ARE NOT ALONE FOUNDATION
951 SW 57 AVENUE
MIAMI, FL 33144
PHONE 786-393-1523
tanafoundation@hotmail.com
barbyganesh@gmail.com
951 SW 57 AVENUE
MIAMI, FL 33144
PHONE 786-393-1523
tanafoundation@hotmail.com
barbyganesh@gmail.com
MEMBERS AND STAFF
TANA FOUNDATION
PRESIDENT: BARBY GANESH- USA
RAJEEV SHARMA INDIA
SHINIVA TIPPANNA INDIA
YASH SIGNH INDIA
SHAKIL SHAIKH INDIA
LISETTE VILLA USA
DANIEL RAMOS NICARAGUA
EDDY PEREZ USA
MANDY GANESH
PRESIDENT: BARBY GANESH- USA
RAJEEV SHARMA INDIA
SHINIVA TIPPANNA INDIA
YASH SIGNH INDIA
SHAKIL SHAIKH INDIA
LISETTE VILLA USA
DANIEL RAMOS NICARAGUA
EDDY PEREZ USA
MANDY GANESH

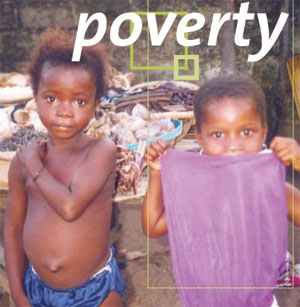 HUNGER AND WORLD POVERTY
HUNGER AND WORLD POVERTYAbout 25,000 people die every day of hunger or hunger-related causes, according to the United Nations. This is one person every three and a half seconds, as you can see on this display. Unfortunately, it is children who die most often.
 Quality of life through health improvement
Quality of life through health improvement• Community health education
• Environment and ecological promotion
• Nutrition education cum services
• Immunization
• Reproductive and child health program
• Coordination with Government Primary Health Centers.
• Periodical medical check-ups and treatment with referral services
• Training for grass root health workers
FIGHT AGAINST CANCER
Mon, 12th September, 2011
They Are Not Alone Foundation before writing this blog is sharing this Story of one of a victim of Cancer-“Carla wakes up one morning feeling that something is wrong. She has been having headaches, but not of the normal, take-a-pill-and-relax type. These headaches come with a sort of numbness, and now she notices some other things that aren’t as they should be. There are bruises on her back that she can’t explain; her gums have been going pale; and she’s very, very tired. She goes to her doctor, but he can’t tell her what’s wrong. Try some aspirin, he says; maybe it’s a migraine. The aspirin doesn’t help, so she finally asks for some blood tests and soon she winds up at Massachusetts General Hospital, in Boston, where a young and talented physician gives her the preliminary diagnosis: acute lymphoblastic leukemia (A.L.L.). Carla knows nothing about lymphoblasts, or why she’s going to have to have a bone-marrow sample taken, but she knows about leukemia. It’s cancer of the blood. She’s terrified, and she may not be in a state of mind to take in the oncologist’s reassurance that A.L.L. is “often curable.”
Carla now enters not just a cancer ward but a cancer world. The ward is what the sociologist Erving Goffman once called a “total institution,” like asylums, armies, prisons, monasteries, and Oxbridge colleges—an institution that strips you of your identity and equips you with a new one. She’s given a case number, a bracelet, a hospital gown. Some of her physicians will know her name and what she was before becoming a cancer patient, and some will not. Her chemotherapy ward is an environment made sterile in order to protect her soon to be therapeutically devastated immune system from infection, so her relations with family and friends are reconfigured along with the rhythms of her days and weeks. She’s now a case.”
Cancer has always been with us, but not always in the same way. Its care and management have differed over time, of course, but so, too, have its identity, visibility, and meanings. Pick up the thread of history at its most distant end and we have cancer the crab—so named either because of the ramifying venous processes spreading out from a tumor or because its pain is like the pinch of a crab’s claw. Premodern cancer is a lump, a swelling that sometimes breaks through the skin in ulcerations producing foul-smelling discharges. The ancient Egyptians knew about many tumors that had a bad outcome, and the Greeks made a distinction between benign tumors and malignant ones. In the second century A.D., Galen reckoned that the cause was systemic, an excess of melancholy or black bile, one of the body’s four “humors,” brought on by bad diet and environmental circumstances. Ancient medical practitioners sometimes cut tumors out, but the prognosis was known to be grim. Describing tumors of the breast, an Egyptian papyrus from about 1600 B.C. concluded: “There is no treatment.”
The experience of cancer has always been terrible, but, until modern times, its mark on the culture has been light. In the past, fear coagulated around other ways of dying: infectious and epidemic diseases (plague, smallpox, cholera, typhus, typhoid fever); “apoplexies” (what we now call strokes and heart attacks); and, most notably in the nineteenth century, “consumption” (tuberculosis). The agonizing manner of cancer death was dreaded, but that fear was not centrally situated in the public mind—as it now is. This is one reason that the medical historian Roy Porter wrote that cancer is “the modern disease .
At one time, it was thought that cancer was a “disease of civilization,” belonging to much the same causal domain as “neurasthenia” and diabetes, the former a nervous weakness believed to be brought about by the stress of modern life and the latter a condition produced by bad diet and indolence.
Cancer is “the modern disease” not just because we understand it in radically new ways but also because there’s a lot more cancer about. For some cancers, the rise in incidence is clearly connected with things that get into our bodies that once did not—the causal link between smoking and lung cancer being the most spectacular example. But the rise in cancer mortality is, in its way, very good news: as we live longer, and as many infectious and epidemic diseases have ceased to be major causes of death, so we become prone to maladies that express themselves at ages once rarely attained. At the beginning of the twentieth century, life expectancy at birth in America was 47.3 years, and in the middle of the nineteenth century it was less than forty. The median age at diagnosis for breast cancer in the United States is now sixty-one; for prostate cancer it is sixty-seven; for colorectal cancer it’s seventy. “Cancer has become the price of modern life,” an epidemiologist recently wrote: in the U.S., about half of all men and about a third of women will contract cancer in their lifetime; cancer now ranks just below heart disease as a cause of death in the U.S. But in low-income countries with shorter life expectancies it doesn’t even make the top ten.
There are basically three ways to treat cancer: we can cut it out surgically; we can burn it up with radiation; and we can poison it by suffusing the body with cytotoxic chemicals that knock out cancer cells without such extensive damage to normal cells that the attempted cure kills. The therapeutic triad can be combined in any number of ways. The fight is hard and the assessment of progress is not easy, but it would be understandable for a modern oncologist to celebrate recent progress and condescend to the knowledge and the therapies of his forebears.
But it’s hard to wage a war against a poorly defined enemy. If the enemy doesn’t define itself, then we can configure the enemy we need for the war that we want to fight. That’s what happened with the War on Cancer. on Cancer resembles less, say, the war on Nazi Germany than the War on Terror.
Most cancer researchers in the nineteen-seventies already understood that cancer is diverse, and the research and clinical care of the following decades gave that diversity greater clarity and texture, implicating a bewildering range of underlying mechanisms. Knowing that all cancers were malignant neoplasms could take cancer care only so far. Turning the patient’s body into something like a free-fire zone wasn’t working, and, by the eighties, it was widely recognized that what the oncologist Guy Faguet has called the “cell-kill paradigm” of chemotherapy had reached its limits. What was needed was a way to engage not just rapidly dividing cells but specifically cancerous cells. We could not get to that goal without a far better understanding of underlying cellular and genetic disease mechanisms. Cancer science and cancer therapy could no longer be kept separate.
A world in which cancer is normalized as a manageable chronic condition would be a wonderful thing, but a risk-factor world in which we all think of ourselves as precancerous would not. It might decrease the incidence of some forms of malignancy while hugely increasing the numbers of healthy people under medical treatment. It would be a strange victory in which the price to be paid for checking the spread of cancer through the body is its uncontrolled spread through the culture. They Are Not Alone Foundation is dedicated towards building an awareness and availing treatment to the poorest economy people who feel there’s no cure for this disease. Together we all can save million on lives who are on the verge of death due to non-treatment in early stages. We all together can make the difference by our little worthy contribution even. We all are borned as Human to act as Human. Be with us in this FIGHT AGAINST CANCER by being part of our event of September “Fight against Cancer”. Kindly visit www.foundationtana.org and make our part today by donating amount of our wish to help People for Surviving and getting rid of cancer in early stages treatment.
Kindest Regards:-
Barby Ganesh
President-They Are Not Alone Foundation
Miami-33144,Florida
Website-www.foundationtana.org
Email-tanafoundation@hotmail.com
barbyganesh@gmail.com
Carla now enters not just a cancer ward but a cancer world. The ward is what the sociologist Erving Goffman once called a “total institution,” like asylums, armies, prisons, monasteries, and Oxbridge colleges—an institution that strips you of your identity and equips you with a new one. She’s given a case number, a bracelet, a hospital gown. Some of her physicians will know her name and what she was before becoming a cancer patient, and some will not. Her chemotherapy ward is an environment made sterile in order to protect her soon to be therapeutically devastated immune system from infection, so her relations with family and friends are reconfigured along with the rhythms of her days and weeks. She’s now a case.”
Cancer has always been with us, but not always in the same way. Its care and management have differed over time, of course, but so, too, have its identity, visibility, and meanings. Pick up the thread of history at its most distant end and we have cancer the crab—so named either because of the ramifying venous processes spreading out from a tumor or because its pain is like the pinch of a crab’s claw. Premodern cancer is a lump, a swelling that sometimes breaks through the skin in ulcerations producing foul-smelling discharges. The ancient Egyptians knew about many tumors that had a bad outcome, and the Greeks made a distinction between benign tumors and malignant ones. In the second century A.D., Galen reckoned that the cause was systemic, an excess of melancholy or black bile, one of the body’s four “humors,” brought on by bad diet and environmental circumstances. Ancient medical practitioners sometimes cut tumors out, but the prognosis was known to be grim. Describing tumors of the breast, an Egyptian papyrus from about 1600 B.C. concluded: “There is no treatment.”
The experience of cancer has always been terrible, but, until modern times, its mark on the culture has been light. In the past, fear coagulated around other ways of dying: infectious and epidemic diseases (plague, smallpox, cholera, typhus, typhoid fever); “apoplexies” (what we now call strokes and heart attacks); and, most notably in the nineteenth century, “consumption” (tuberculosis). The agonizing manner of cancer death was dreaded, but that fear was not centrally situated in the public mind—as it now is. This is one reason that the medical historian Roy Porter wrote that cancer is “the modern disease .
At one time, it was thought that cancer was a “disease of civilization,” belonging to much the same causal domain as “neurasthenia” and diabetes, the former a nervous weakness believed to be brought about by the stress of modern life and the latter a condition produced by bad diet and indolence.
Cancer is “the modern disease” not just because we understand it in radically new ways but also because there’s a lot more cancer about. For some cancers, the rise in incidence is clearly connected with things that get into our bodies that once did not—the causal link between smoking and lung cancer being the most spectacular example. But the rise in cancer mortality is, in its way, very good news: as we live longer, and as many infectious and epidemic diseases have ceased to be major causes of death, so we become prone to maladies that express themselves at ages once rarely attained. At the beginning of the twentieth century, life expectancy at birth in America was 47.3 years, and in the middle of the nineteenth century it was less than forty. The median age at diagnosis for breast cancer in the United States is now sixty-one; for prostate cancer it is sixty-seven; for colorectal cancer it’s seventy. “Cancer has become the price of modern life,” an epidemiologist recently wrote: in the U.S., about half of all men and about a third of women will contract cancer in their lifetime; cancer now ranks just below heart disease as a cause of death in the U.S. But in low-income countries with shorter life expectancies it doesn’t even make the top ten.
There are basically three ways to treat cancer: we can cut it out surgically; we can burn it up with radiation; and we can poison it by suffusing the body with cytotoxic chemicals that knock out cancer cells without such extensive damage to normal cells that the attempted cure kills. The therapeutic triad can be combined in any number of ways. The fight is hard and the assessment of progress is not easy, but it would be understandable for a modern oncologist to celebrate recent progress and condescend to the knowledge and the therapies of his forebears.
But it’s hard to wage a war against a poorly defined enemy. If the enemy doesn’t define itself, then we can configure the enemy we need for the war that we want to fight. That’s what happened with the War on Cancer. on Cancer resembles less, say, the war on Nazi Germany than the War on Terror.
Most cancer researchers in the nineteen-seventies already understood that cancer is diverse, and the research and clinical care of the following decades gave that diversity greater clarity and texture, implicating a bewildering range of underlying mechanisms. Knowing that all cancers were malignant neoplasms could take cancer care only so far. Turning the patient’s body into something like a free-fire zone wasn’t working, and, by the eighties, it was widely recognized that what the oncologist Guy Faguet has called the “cell-kill paradigm” of chemotherapy had reached its limits. What was needed was a way to engage not just rapidly dividing cells but specifically cancerous cells. We could not get to that goal without a far better understanding of underlying cellular and genetic disease mechanisms. Cancer science and cancer therapy could no longer be kept separate.
A world in which cancer is normalized as a manageable chronic condition would be a wonderful thing, but a risk-factor world in which we all think of ourselves as precancerous would not. It might decrease the incidence of some forms of malignancy while hugely increasing the numbers of healthy people under medical treatment. It would be a strange victory in which the price to be paid for checking the spread of cancer through the body is its uncontrolled spread through the culture. They Are Not Alone Foundation is dedicated towards building an awareness and availing treatment to the poorest economy people who feel there’s no cure for this disease. Together we all can save million on lives who are on the verge of death due to non-treatment in early stages. We all together can make the difference by our little worthy contribution even. We all are borned as Human to act as Human. Be with us in this FIGHT AGAINST CANCER by being part of our event of September “Fight against Cancer”. Kindly visit www.foundationtana.org and make our part today by donating amount of our wish to help People for Surviving and getting rid of cancer in early stages treatment.
Kindest Regards:-
Barby Ganesh
President-They Are Not Alone Foundation
Miami-33144,Florida
Website-www.foundationtana.org
Email-tanafoundation@hotmail.com
barbyganesh@gmail.com
Double click here to edit this text.